
Is Sermorelin Safe? What You Need to Know Before Starting Treatment
Published on:
Updated on:
People are asking...
How about stacking TRT with peptide therapy. Are Sermorelin, Tesamorelin, or CJC w/ Ipamorelin actually safe to use with TRT? What are the real benef...
These are perfectly reasonable options. Currently, licensed providers can prescribe Sermorelin, though not long ago it was permissible to work with the other peptides you mentioned as well. Many men h... See Full Answer
Do you offer peptides and if so can you talk a little bit about which ones you offer and the possible benefits?...
Yes — providers on the AlphaMD platform can prescribe certain peptides, though the selection is more tightly focused than a full on peptide provider. This is because prescribing is limited to peptides... See Full Answer
What are the best peptides to pair with TRT for getting lean?...
In terms of current official pharmacy offerings, providers often recommend Sermorelin as a good boost. Anecdotally, Ipamorelin / CJC with or without dac is often described as a solid peptide for fitne... See Full Answer
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
Most people asking whether sermorelin is safe are already doing something right - they are asking questions before starting, not after. That instinct matters, because sermorelin is a legitimate medical treatment with a real track record, and understanding both its strengths and its limits is the foundation of using it responsibly.
What Sermorelin Actually Is (and Why It Is Not the Same as Growth Hormone)
Sermorelin is a synthetic peptide made up of 29 amino acids. It is modeled after the first 29 amino acids of human growth hormone-releasing hormone (GHRH), the signaling molecule your hypothalamus naturally produces to tell your pituitary gland to release growth hormone. It is, in fact, the shortest synthetic version of GHRH that retains the full biological activity of the natural hormone.
This distinction - between sermorelin and growth hormone itself - is not a technicality. It is the most important thing to understand about how this treatment works.
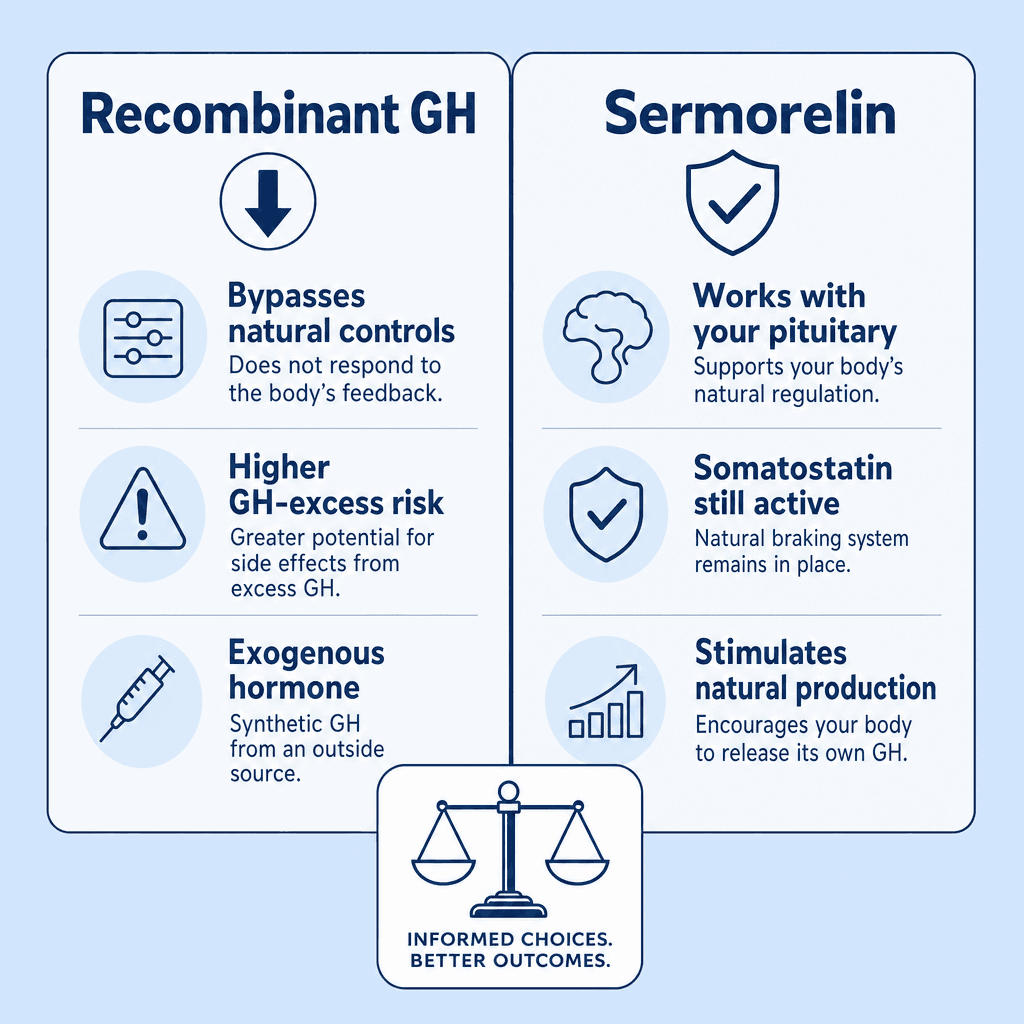
When you take recombinant human growth hormone (rhGH), you are introducing an external hormone directly into your body. When you use sermorelin, you are delivering a signal to your pituitary gland and asking it to do its own job. The pituitary then produces and releases growth hormone on its own, in its own pulsatile pattern, the way the body naturally does it. That distinction shapes nearly everything about sermorelin's safety profile.
Sermorelin received FDA approval in 1997 under the brand name Geref for stimulating growth in children with idiopathic growth hormone deficiency. It was also approved as a diagnostic agent for confirming adult growth hormone deficiency. The manufacturer later withdrew it from the pediatric growth market - not over safety concerns - but because children requiring active growth promotion often need higher GH concentrations than sermorelin alone can generate. Somatropin (direct injectable GH) became the more commercially practical option for that specific indication.
For adults, however, that same "limitation" becomes a feature. Physiologically appropriate, lower-level stimulation of the body's own GH production is precisely the goal.
The Self-Regulating Mechanism That Sets Sermorelin Apart
One of the most clinically significant aspects of sermorelin's safety profile is what happens when growth hormone rises too high. The body has a built-in inhibitory neurohormone called somatostatin that acts as a natural brake on GH secretion. When GH levels climb past a physiologic range, somatostatin activates and suppresses further release.
Because sermorelin works through the pituitary rather than bypassing it, this feedback loop remains intact. Researchers have noted that achieving a true GH overdose with sermorelin is, in the words of one widely cited review, "difficult if not impossible to achieve" - a stark contrast to injecting rhGH directly, where that protective brake is essentially removed from the equation.
This does not mean monitoring is unnecessary. It means the physiologic guardrails are working as designed. Oversight is still required to confirm they are.
Research published by Harvard Medical School's Neuroendocrine Unit at Massachusetts General Hospital found that GHRH therapy significantly reduces visceral adipose tissue, improves lipid profiles including triglycerides, and reduces cardiovascular risk markers such as carotid intima-media thickness and C-reactive protein. These findings suggest that beyond the hormonal effects, sermorelin may carry meaningful metabolic benefits - particularly in individuals with excess visceral fat, a group in which functional growth hormone deficiency is surprisingly common.
Why People Are Prescribed Sermorelin
Growth hormone secretion declines naturally with age. This decline, sometimes called somatopause, is associated with changes in body composition, reduced muscle mass, increased visceral fat, lower energy, disrupted sleep, and other signs that many people associate with "just getting older."
For adults experiencing these changes - particularly when clinical evaluation suggests growth hormone insufficiency - sermorelin may be prescribed as a way to support the body's own GH production rather than replace it externally. Because sermorelin works through the pituitary and may actually help preserve and restore pituitary function over time, some clinicians view it as a more physiologically aligned option than direct GH replacement.
It is worth noting that adult use of sermorelin is considered off-label, meaning the FDA has not granted a current active approval for this specific indication. Prescribing sermorelin for adults is not prohibited by federal law - unlike rhGH, which faces strict federal restrictions limiting adult use to AIDS wasting and diagnosed growth hormone deficiency. Sermorelin's regulatory flexibility is real, but off-label use also means the prescribing physician carries greater responsibility for patient selection and monitoring.
Common Side Effects and What the Clinical Record Shows
The side effect profile for sermorelin is generally mild. The Mayo Clinic's drug monograph identifies pain, redness, or swelling at the injection site as the most commonly documented adverse effect. Rare side effects include itching, trouble swallowing, dizziness, flushing, headache, sleepiness, and restlessness.
A peer-reviewed review published in BioDrugs concluded that both intravenous single-dose and repeated once-daily subcutaneous doses of sermorelin are well tolerated, with transient facial flushing and injection-site pain being the most commonly reported events.
What about the side effects associated with excess growth hormone - joint pain, fluid retention, carpal tunnel syndrome? These do appear in some individuals, but at notably lower rates than with rhGH. Because sermorelin's pulsatile GH release more closely mirrors how the body naturally secretes growth hormone, the "square wave" constant-exposure effect of injected rhGH is avoided. Joint pain and peripheral edema have been reported in a limited number of subjects across GHRH studies.
On the question of cancer risk, no increased incidence of malignancy has been observed in GHRH clinical studies to date. Long-term Phase 4 post-market surveillance is ongoing, and this remains an area where patients with a personal or family history of hormone-sensitive cancers should discuss their specific situation carefully with a physician.
Insulin sensitivity is another nuance worth understanding. Some studies show a transient, initial worsening of insulin sensitivity with GHRH therapy, followed by a return to baseline with continued treatment. This is a meaningfully different profile from rhGH, which consistently and persistently worsens glucose tolerance. That said, individuals with diabetes or pre-diabetes require closer monitoring and careful clinical judgment.
Who Should Be Cautious or Avoid Treatment Entirely
Sermorelin is not appropriate for everyone. Several categories of patients warrant extra caution or should avoid it altogether.
Active malignancy is a firm contraindication. Growth hormone has known mitogenic (cell-growth-promoting) properties, and stimulating GH in someone with active cancer is not considered appropriate.
Hypothyroidism is a frequently overlooked issue. An underactive thyroid can interfere with sermorelin's effectiveness at the pituitary level, reducing or blunting the expected response. Thyroid status should be evaluated before and during treatment - not just as a screening step, but as an ongoing part of management.
Obesity, particularly central or visceral obesity, creates a more complex picture. Elevated visceral fat is associated with reduced GH secretion, and research suggests this relationship can become self-reinforcing. Interestingly, functional GH deficiency related to obesity may be partially reversible with weight loss alone. Clinicians must distinguish between true pituitary-axis deficiency and functional suppression driven by metabolic factors.
Pregnancy, active pituitary tumors, known hypersensitivity to sermorelin or its components, and any condition creating elevated intracranial pressure also require careful evaluation. Patients already receiving systemic corticosteroids should be aware that these can blunt the pituitary's response to GHRH stimulation.
Practical Questions to Ask Before You Start
Before beginning sermorelin therapy, a well-prepared patient should feel comfortable asking their provider several direct questions. What baseline labs are being obtained, and what do the results suggest about your GH axis function? How will IGF-1 levels be monitored during treatment, and at what interval? What specific symptoms would indicate a need to pause or stop treatment? Has your thyroid function been assessed? Are there any concurrent medications, supplements, or health conditions that could interact with or limit the response?
IGF-1 monitoring during treatment is not optional - it is a critical safety requirement. Ensuring that growth hormone remains within the physiologic range, rather than climbing into supraphysiologic territory, is the primary safety check for ongoing therapy.
The injection itself is subcutaneous, meaning it goes into the tissue just beneath the skin rather than into muscle or a vein. Sites should be rotated across different areas to reduce localized irritation, and the medication requires refrigeration. Patients should receive clear guidance on proper technique from their prescribing provider.
Realistic Expectations: What Sermorelin Can and Cannot Do
Sermorelin is not a shortcut to dramatic transformation. Patients who approach it expecting rapid or dramatic results are likely to be disappointed - and may also be at higher risk of seeking higher doses or unsupervised sources, both of which carry real risks.
What the clinical evidence does support, in appropriately selected adults with meaningful GH axis decline, is a gradual improvement in body composition over months, better sleep quality (growth hormone is primarily released during deep sleep), improved energy and recovery, and potentially favorable metabolic shifts including reductions in visceral fat. These changes tend to become more apparent after several months of consistent, supervised use.
What sermorelin cannot do is reverse all aspects of aging, compensate for poor lifestyle habits, or substitute for comprehensive care. It is one tool - a physiologically targeted one - that functions best when combined with adequate sleep, sensible nutrition, and an overall health plan developed with a qualified clinician.
Treatment decisions should always be individualized. Hormone optimization is not a one-size-fits-all field. Factors like age, baseline hormone status, thyroid function, body composition, metabolic health, and personal goals all factor into whether sermorelin is appropriate and, if so, what a reasonable treatment plan looks like.
Making an Informed Decision with the Right Medical Support
The safety record for sermorelin, across both clinical literature and real-world medical use, is genuinely reassuring. It is a well-studied peptide with a self-regulating mechanism, a mild side effect profile, and meaningful physiologic advantages over direct GH replacement for many adults. But reassuring is not the same as risk-free, and no serious clinician would present it that way.
The path to using sermorelin safely runs through proper screening, honest clinical evaluation, ongoing monitoring, and a provider who treats you as an individual rather than applying a protocol. If you are considering whether this treatment makes sense for your situation, that conversation belongs in a clinical setting - not a forum, not a supplement store.
Through AlphaMD, eligible patients connect with licensed providers who evaluate whether sermorelin is appropriate and oversee individualized care and monitoring from the start. Informed patients who ask the right questions and work with the right providers are the ones who get the best outcomes - and the safest experience.
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
People are asking...
How about stacking TRT with peptide therapy. Are Sermorelin, Tesamorelin, or CJC w/ Ipamorelin actually safe to use with TRT? What are the real benef...
These are perfectly reasonable options. Currently, licensed providers can prescribe Sermorelin, though not long ago it was permissible to work with the other peptides you mentioned as well. Many men h... See Full Answer
Do you offer peptides and if so can you talk a little bit about which ones you offer and the possible benefits?...
Yes — providers on the AlphaMD platform can prescribe certain peptides, though the selection is more tightly focused than a full on peptide provider. This is because prescribing is limited to peptides... See Full Answer
What are the best peptides to pair with TRT for getting lean?...
In terms of current official pharmacy offerings, providers often recommend Sermorelin as a good boost. Anecdotally, Ipamorelin / CJC with or without dac is often described as a solid peptide for fitne... See Full Answer
Get $30 off your first month’s order
Enter your email address now to receive $30 off your first month’s cost, other discounts, and additional information about TRT.
Legal Disclaimer
This website is a repository of publicly available information and is not intended to form a physician-patient relationship with any individual. The content of this website is for informational purposes only. The information presented on this website is not intended to take the place of your personal physician's advice and is not intended to diagnose, treat, cure, or prevent any disease. Discuss this information with your own physician or healthcare provider to determine what is right for you. All information is intended for your general knowledge only and is not a substitute for medical advice or treatment for specific medical conditions. The information contained herein is presented in summary form only and intended to provide broad consumer understanding and knowledge. The information should not be considered complete and should not be used in place of a visit, phone or telemedicine call, consultation or advice of your physician or other healthcare provider. Only a qualified physician in your state can determine if you qualify for and should undertake treatment.