
Dehydration Is Inflating Your Hematocrit Number - And Most Men on TRT Don't Know It
Published on:
Updated on:
People are asking...
Men living at high altitudes often have raised hematocrit levels and this is deemed normal/safe/ok. Men on TRT who get above 50% PCV are usually giv...
This is an excellent question, which requires a pretty complex answer. But the basics lie in the differences between chronic hypoxia induced erythrocytosis and exogenous testosterone induced erythrocy... See Full Answer
How dangerous is high hematorcrit?...
There are some studies that show it can increase cardiovascular issues, though you'd tend to notice some of the symptoms if it was induced from starting TRT. Brain fog & additional headaches are prett... See Full Answer
If guys in places like Colorado have higher hematocrit levels from being at higher altitudes, why do guys on TRT have to donate blood when their hemat...
Mostly because of what it does to you & how each person is different. Their bodies may be doing that based on the strain of their environment & then utilizing the changes to better function. Someone n... See Full Answer
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
Your doctor flags a high hematocrit on your TRT labs, and suddenly you're worried about blood clots, dose adjustments, or worse. But before drawing any conclusions, there's a question that almost never gets asked first: how hydrated were you when that blood was drawn?
For men on testosterone replacement therapy, hematocrit is one of the most closely watched numbers in the entire lab panel. It's also one of the most misunderstood, because a single variable that has nothing to do with your testosterone dose can push that number into concerning territory overnight. That variable is dehydration, and it's far more common, and far more influential, than most men on TRT realize.
What Hematocrit Actually Measures, and Why TRT Changes the Equation
Hematocrit is the percentage of your blood volume made up of red blood cells. Think of your blood as a mixture of two things: the cellular components (mostly red blood cells) and the liquid they float in, which is called plasma. Hematocrit simply tells you what fraction of the total mixture is cells versus fluid.
Testosterone is well known for stimulating the production of red blood cells through a process involving erythropoietin, a hormone that signals the bone marrow to ramp up output. This is why men on TRT are monitored for elevated hematocrit. A genuinely high red blood cell mass can thicken the blood and raise the theoretical risk of cardiovascular events over time. That concern is real, clinically recognized, and worth taking seriously.
But here's what often gets overlooked: hematocrit is a ratio, not a direct count of red blood cells. When the plasma volume drops, even if your actual red blood cell mass stays exactly the same, the ratio shifts upward. The cells haven't multiplied. The fluid they're suspended in has simply decreased. The result looks identical on a standard lab report, and without context, it's easy to misinterpret.
The Difference Between Real Polycythemia and a Dehydrated Blood Draw
Clinicians use terms like "absolute erythrocytosis" to describe a true increase in red blood cell mass, and "relative erythrocytosis" or "hemoconcentration" to describe an elevated hematocrit caused by reduced plasma volume. Both will produce a high number on your lab report. Only one of them represents an actual increase in the cells circulating through your arteries.
This distinction matters enormously in clinical decision-making. A true rise in red blood cell mass from long-term TRT use is a legitimate medical concern that warrants evaluation and potentially a change in management. An artificially concentrated blood sample taken from a mildly dehydrated man after a morning fast and two cups of coffee tells a very different story, one that shouldn't automatically trigger the same response.
The challenge is that a standard complete blood count, which is how hematocrit is typically measured, cannot distinguish between the two on its own. Context, timing, and patient history have to fill that gap.
The Everyday Dehydration Triggers TRT Patients Should Know About
Most men don't think of themselves as dehydrated unless they're dizzy and craving water after a long run. But mild dehydration, the kind that quietly reduces plasma volume without triggering obvious symptoms, is remarkably common and surprisingly easy to stumble into before a morning lab appointment.
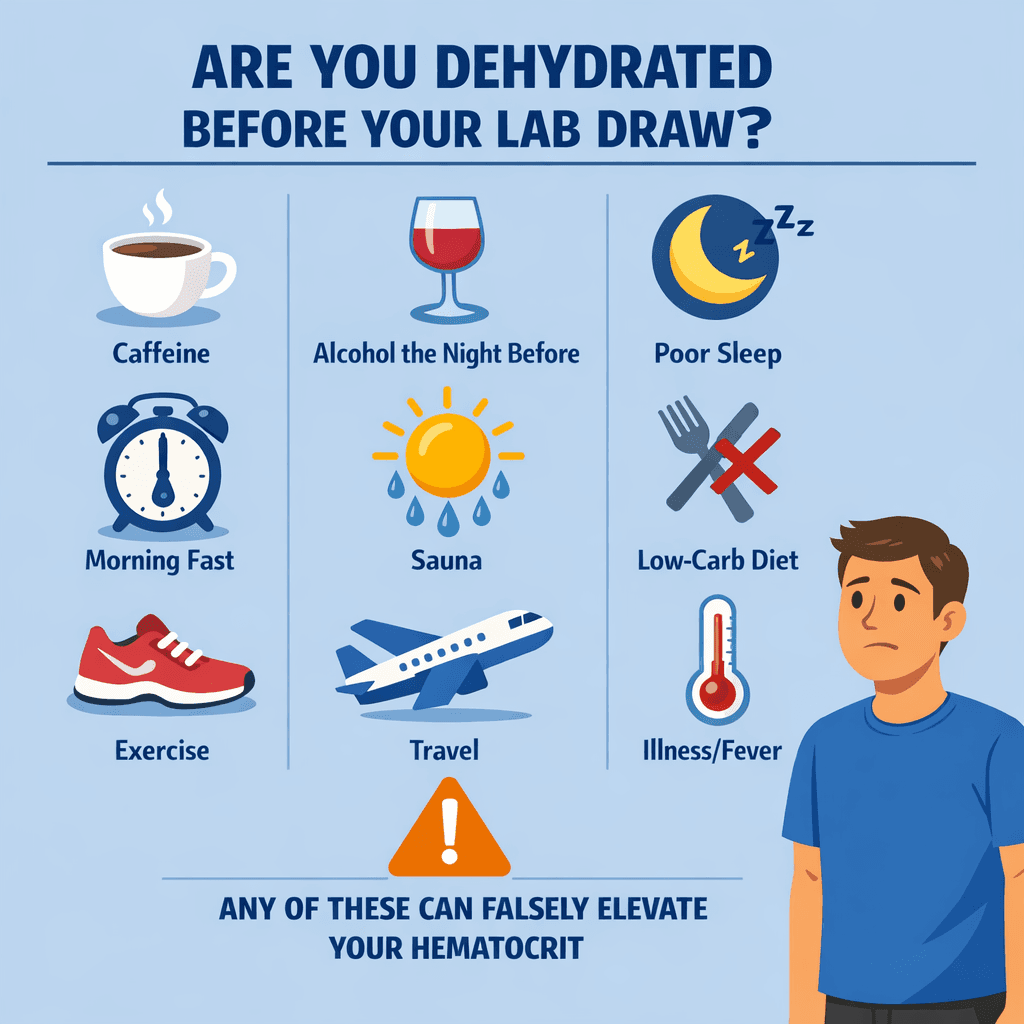
Intense exercise, particularly the day before a blood draw, can produce fluid losses that aren't fully replaced by the next morning. Saunas and steam rooms, popular for recovery among active men, accelerate fluid loss through sweat in a way that's easy to underestimate. Alcohol is a diuretic, meaning it actively drives fluid out of the body, and even moderate consumption the evening before a lab can leave plasma volume lower by morning. Illness involving fever, vomiting, or diarrhea creates obvious and rapid dehydration, but many men don't think to reschedule labs during or shortly after being sick.
Travel, especially long flights in dry cabin air, is a frequently underestimated dehydrating experience. Low-carb and ketogenic diets, which are popular among men focused on body composition, promote excretion of water and electrolytes through reduced glycogen storage, keeping many men in a chronically lower state of hydration than they realize. High caffeine intake acts as a mild diuretic. Poor or disrupted sleep affects fluid regulation in ways that aren't fully appreciated by most people outside of clinical circles.
Any one of these factors, let alone several of them stacked together, can meaningfully reduce plasma volume and push hematocrit upward on a lab report without a single new red blood cell being produced.
Why Morning Fasting Labs Are Particularly Vulnerable to This Effect
Standard lab protocols typically require fasting before bloodwork, which is appropriate for accurate glucose and lipid readings. But fasting also means no fluid intake for a significant stretch of time, usually from the evening before through the morning draw. For most people, sleep itself is a mild dehydrating event. You're breathing out moisture for six to eight hours without replacing it.
Add a cup or two of coffee in the morning, which many men drink before labs without thinking much about it, and you've layered a diuretic effect on top of an already-reduced fluid state. Add a morning workout before the appointment, and the problem compounds further. Add a sauna session the evening before, a few drinks the night prior, or a night of poor sleep, and the blood sample being drawn may reflect a significantly hemoconcentrated state that simply isn't representative of normal, well-hydrated physiology.
This doesn't mean fasting labs are flawed or that the results are useless. It means that the conditions surrounding the draw have real physiological consequences, and those conditions are almost never documented or accounted for in the result interpretation unless the patient raises them.
How to Approach Lab Timing with Hydration in Mind
The goal isn't to game your results or mask a genuine problem. It's to make sure the reading you get actually reflects your biology under normal conditions, rather than a snapshot of a dehydrated morning you'll never think about again.
In general terms, consistent and adequate hydration in the day or two leading up to a blood draw gives a more accurate picture. Avoiding particularly dehydrating activities, like intense training, alcohol, or sauna use, in the 24 hours before labs can reduce unnecessary variation. Plain water in the morning before a fasting draw, in amounts that feel normal for your routine, is generally not prohibited for standard hematocrit testing, though it's worth confirming with your lab or provider what your specific draw requires.
Being transparent with your clinician about any of the factors mentioned above is genuinely useful information. If you were traveling, fighting off a bug, drinking more than usual, or sweating heavily before your draw, say so. That context can change how a borderline result gets interpreted, and whether a repeat test under more controlled conditions is worth ordering before any clinical decisions are made.
When Dehydration Isn't the Whole Answer
It would be a mistake to treat dehydration as a convenient explanation that explains away every high hematocrit reading. Persistent elevation across multiple draws, taken under reasonable conditions, deserves genuine medical attention.
Several factors beyond TRT dose can contribute to a true rise in red blood cell production. Undiagnosed or undertreated sleep apnea is one of the most commonly overlooked contributors. The repeated drops in oxygen during apnea episodes stimulate the body to produce more red blood cells as a compensatory response, often pushing hematocrit upward independent of testosterone levels. Smoking has a similar physiological effect. Living at high altitude chronically reduces ambient oxygen, triggering the same compensatory mechanism. Certain underlying conditions affecting kidney function, bone marrow, or oxygen sensing can also drive erythrocytosis.
A high hematocrit on TRT isn't automatically a dose problem, and it isn't automatically a dehydration artifact either. It's a finding that warrants context, follow-up, and a clinician who understands the full picture.
The Conversation Worth Having with Your Provider
If your hematocrit comes back elevated, the most useful thing you can do is resist the urge to either panic or dismiss it, and instead bring everything relevant to your next appointment. When was the draw taken? Had you eaten or drunk anything? Did you exercise the day before? Were you traveling, under stress, or recovering from something? These details aren't excuses. They're clinical context that a thoughtful provider will actually want.
In some cases, simply repeating the test under better-controlled conditions is a reasonable starting point, particularly if there's reason to believe dehydration may have been a factor. In other cases, additional workup may be appropriate. That determination belongs in the hands of a qualified clinician, not a forum thread or a self-treatment decision made in frustration.
Self-managing a high hematocrit reading, whether by reducing your own dose, seeking unsupervised phlebotomy, or avoiding follow-up altogether, bypasses the diagnostic process and can lead to poor outcomes in either direction.
Hydration, Context, and the Limits of a Single Number
A hematocrit reading is not a verdict. It's a data point, and like every data point, its meaning depends on the conditions under which it was collected. For men on TRT, where that number carries clinical weight and can influence treatment decisions, understanding the role of hydration isn't optional knowledge. It's foundational.
Your plasma volume fluctuates throughout the day and across days based on how much you drink, sweat, sleep, eat, and move. A blood draw captures a single moment in that constantly shifting state. Taking that snapshot at a dehydrated moment and treating it as your definitive hematocrit is like weighing yourself after a long run and concluding you've lost body fat.
Teams like AlphaMD are built around exactly this kind of nuanced TRT monitoring, combining ongoing lab interpretation with patient education so that men actually understand what their numbers mean and what they don't. The goal isn't to minimize legitimate concerns. It's to make sure clinical decisions get made with accurate information, and that a dehydrated blood draw doesn't lead to an unnecessary intervention for a man whose red blood cell mass is exactly where it should be.
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
People are asking...
Men living at high altitudes often have raised hematocrit levels and this is deemed normal/safe/ok. Men on TRT who get above 50% PCV are usually giv...
This is an excellent question, which requires a pretty complex answer. But the basics lie in the differences between chronic hypoxia induced erythrocytosis and exogenous testosterone induced erythrocy... See Full Answer
How dangerous is high hematorcrit?...
There are some studies that show it can increase cardiovascular issues, though you'd tend to notice some of the symptoms if it was induced from starting TRT. Brain fog & additional headaches are prett... See Full Answer
If guys in places like Colorado have higher hematocrit levels from being at higher altitudes, why do guys on TRT have to donate blood when their hemat...
Mostly because of what it does to you & how each person is different. Their bodies may be doing that based on the strain of their environment & then utilizing the changes to better function. Someone n... See Full Answer
Get $30 off your first month’s order
Enter your email address now to receive $30 off your first month’s cost, other discounts, and additional information about TRT.
Legal Disclaimer
This website is a repository of publicly available information and is not intended to form a physician-patient relationship with any individual. The content of this website is for informational purposes only. The information presented on this website is not intended to take the place of your personal physician's advice and is not intended to diagnose, treat, cure, or prevent any disease. Discuss this information with your own physician or healthcare provider to determine what is right for you. All information is intended for your general knowledge only and is not a substitute for medical advice or treatment for specific medical conditions. The information contained herein is presented in summary form only and intended to provide broad consumer understanding and knowledge. The information should not be considered complete and should not be used in place of a visit, phone or telemedicine call, consultation or advice of your physician or other healthcare provider. Only a qualified physician in your state can determine if you qualify for and should undertake treatment.