Your Total Testosterone Is a Lie. Here's What Actually Matters.
Published on:
Updated on:
People are asking...
It makes no rational sense to me that total testosterone “far more important”…. even for starting dose. When subjects can have the same total testoste...
Maybe think of it a different way. Your FT level varies a lot based on your SHBG and your albumin levels. And since no one knows to what degree your body will respond to TRT, initial dosing, for the T... See Full Answer
I'm 37. I went to a clinic with my complaints and a hormonal test was done: Fsh 2.69mIU/mL Lh 7.28mIU/mL Prolactin 3.95ng/mL Testosterone 18.0nmol...
Your doctors didn’t lie in saying your labs don’t show anything abnormal. But they won’t always because what is “normal” is based on population averages, not what is normal for you. There is a new di... See Full Answer
I did a blood test in February and my doctor only had total testosterone tested. It came back as 339. I knew my doctor wouldn’t even consider prescrib...
So, providers on the AlphaMD platform utilize the updated age related treatment thresholds that were suggested in this study . If you are under age 45, a provider may determine that you qualify for t... See Full Answer
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
Most men who get their testosterone checked walk away with one number and one question: is it normal? That question, while understandable, is almost entirely the wrong one to ask.
Total testosterone is the figure that shows up on a standard lab panel, and for decades it has been treated as the definitive answer to whether a man's hormonal health is on track. The problem is that it isn't. Two men can have identical total testosterone levels and feel completely different - one energetic, motivated, and sharp, the other exhausted, flat, and struggling to recognize himself in the mirror. That gap is not a mystery. It is biology, and understanding it changes everything about how you interpret your results.
The Number on Your Lab Report Is Only Part of the Story
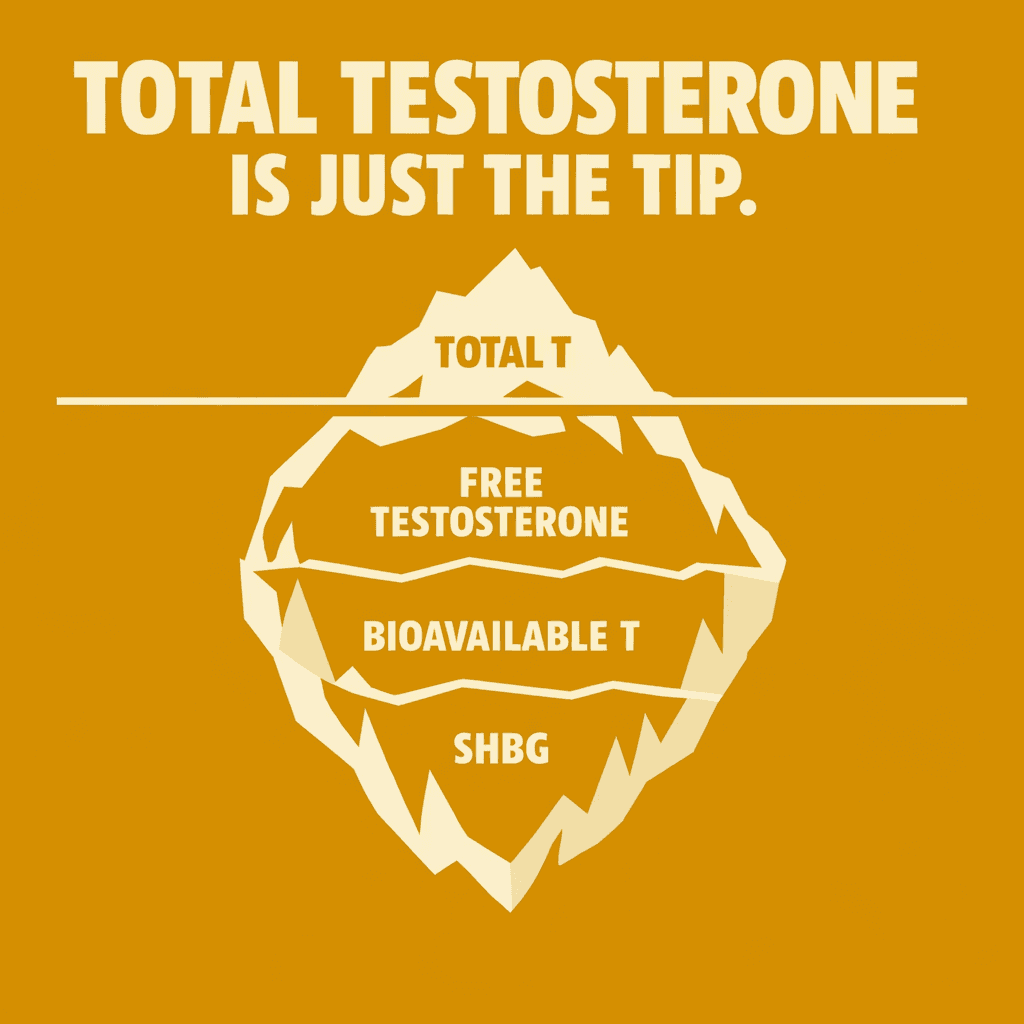
Total testosterone measures all of the testosterone circulating in your blood, regardless of whether your body can actually use it. It is a count of every molecule, but it does not tell you how much of that testosterone is biologically active - how much is actually getting into your cells and doing its job.
Think of it this way: owning a car is not the same as being able to drive it. You might have ten vehicles in your driveway, but if nine of them have no keys, no fuel, or a locked steering wheel, you are getting around on one. Your total testosterone count is the number of cars. What actually moves you forward is something else.
Free and Bioavailable Testosterone: What Your Body Can Actually Use
Testosterone in the bloodstream exists in different states. A portion is tightly bound to a protein called sex hormone-binding globulin, or SHBG. Another portion is loosely bound to albumin, a protein that carries many substances through the blood. The remainder floats freely, unattached to anything.
Free testosterone is that unbound fraction. It is small in percentage terms, but it is the most immediately active form because it can cross directly into cells and exert its effects. Bioavailable testosterone includes both free testosterone and the albumin-bound portion - the logic being that the albumin bond is weak enough that testosterone can detach easily and become available to tissues when needed.
When clinicians talk about whether a man actually has enough functional testosterone, free and bioavailable levels often tell a more accurate story than total testosterone alone. A man with high total testosterone but elevated SHBG may have very little free testosterone - and may feel every bit as symptomatic as someone with clinically low total levels.
SHBG: The Protein That Controls How Much Testosterone You Can Use
SHBG is produced primarily in the liver, and it binds tightly to testosterone (as well as to other hormones like estrogen). Once testosterone is bound to SHBG, it is largely unavailable to tissues. The body cannot use what SHBG has locked away.
Albumin, by contrast, holds testosterone loosely. The binding is weak and reversible, which is why albumin-bound testosterone is generally counted in the bioavailable fraction.
What raises SHBG? Quite a few things, including aging, elevated thyroid hormone levels, certain liver conditions, some medications, and lower body weight. What lowers it? Insulin resistance, obesity, hypothyroidism, and certain other metabolic conditions tend to suppress SHBG - which sounds like it would always be a good thing, but the relationship is more complicated than that. Very low SHBG can reflect underlying metabolic dysfunction that affects hormonal health in other ways.
The takeaway is that SHBG is not just a background variable. It is a central regulator of how much testosterone your body can actually put to use.
Why Your Free Testosterone Can Change Without Your Total Testosterone Budging
Several common factors shift the balance between total and free testosterone, often in ways that show up in symptoms long before they are caught on a basic lab panel.
Age is one of the most consistent drivers. As men get older, SHBG tends to rise. Total testosterone may remain within a "normal" range while free testosterone gradually declines - which is one reason why many men in their forties and fifties feel the effects of lower testosterone without ever being flagged on a standard test.
Body composition and metabolic health matter significantly. Excess body fat, particularly visceral fat around the midsection, is metabolically active tissue. It promotes inflammation, can increase the conversion of testosterone to estrogen through a process called aromatization, and is associated with insulin resistance - a state in which cells become less responsive to insulin. Insulin resistance tends to suppress SHBG, which sounds helpful in isolation, but in the context of broader metabolic disruption, the net effect on hormonal health is rarely favorable.
Thyroid function is another variable that often goes unchecked in men investigating low testosterone symptoms. Thyroid hormones influence SHBG production. An overactive thyroid tends to raise SHBG; an underactive one tends to lower it. Either scenario can distort the picture painted by total testosterone alone.
Liver health is relevant because the liver produces SHBG. Conditions that affect liver function can alter how much SHBG is made, which in turn affects free testosterone levels.
Certain medications - including some commonly prescribed for other conditions - can affect SHBG levels or interfere with hormone production and metabolism. Chronic stress elevates cortisol, which has a well-documented suppressive effect on testosterone production over time. Poor sleep, even in the short term, measurably impacts testosterone levels, particularly the overnight and early morning surge that represents peak production for most men.
None of these factors will show up if the only thing being measured is total testosterone.
Symptoms Are Not Optional Data Points
Lab values exist to support clinical evaluation, not replace it. The experience of low testosterone - low libido, difficulty maintaining erections, persistent fatigue, low motivation, mood changes, difficulty building or maintaining muscle, increased body fat, poor recovery after exercise, disrupted sleep - is real and meaningful regardless of what a single number says.
Two men with the same total testosterone reading may have completely different symptom profiles based on their free testosterone levels, estrogen balance, overall metabolic health, and individual sensitivity. Chasing a specific lab number without accounting for how a man actually feels is an incomplete approach. Equally, assuming symptoms are purely hormonal without a thorough workup ignores the many other factors that can produce similar experiences.
The point is not to dismiss lab work. It is to use it as one piece of a larger, more honest picture.
Why When You Test Matters as Much as What You Test
Testosterone levels are not static. They follow a daily rhythm, typically peaking in the morning and declining through the afternoon and evening. Testing at different times of day can produce meaningfully different results, which is why morning testing is generally preferred.
Acute illness, significant psychological stress, poor sleep in the nights leading up to the test, and even intense exercise can all temporarily suppress testosterone levels. A single low reading taken in the wrong context can be misleading. Conversely, a single normal reading taken under ideal conditions does not rule out a broader pattern of suboptimal hormone function.
Repeat testing, appropriate timing, and looking at trends over time all contribute to a more accurate assessment than any one data point can provide.
What a Complete Hormonal Evaluation Actually Looks Like
A thorough evaluation typically goes well beyond a single testosterone test. Clinicians with expertise in men's hormonal health commonly consider a broader set of markers to build an accurate picture.
SHBG is central, as discussed. Estradiol - the primary form of estrogen - matters because men do produce and require estrogen, and imbalances in either direction can cause symptoms. LH and FSH, hormones produced by the pituitary gland that signal the testes to produce testosterone, help distinguish between primary testicular issues and problems originating higher in the hormonal signaling chain. Prolactin, another pituitary hormone, can suppress testosterone when elevated and is worth evaluating. Thyroid markers provide insight into a gland that influences metabolism and SHBG. A complete metabolic panel and complete blood count round out the picture by flagging liver health, blood sugar regulation, red blood cell status, and other variables that interact with hormonal function.
That list might seem long. The reason it matters is that hormonal health does not exist in isolation - it is embedded in overall physiology, and treating it that way produces better outcomes.
Common Misconceptions Worth Correcting
One persistent belief is that higher testosterone is always better. It is not. Hormones operate within a system, and pushing any single variable to an extreme without attending to the rest of the system creates imbalances. More is not inherently better; appropriate and functional is the actual goal.
Another misconception is that one lab test tells the whole story. It does not, for all the reasons covered above.
TRT is not the only possible solution for men experiencing symptoms of low testosterone. Lifestyle factors - particularly sleep quality, resistance training, body composition, and metabolic health - have real and measurable effects on hormonal status. For some men, addressing these factors moves the needle significantly. Others have underlying issues that lifestyle changes alone will not resolve, and medical intervention becomes a reasonable conversation. The distinction between those situations is exactly why evaluation by a qualified clinician matters.
Finally, the supplement market is full of products that claim to naturally boost testosterone. While some nutrients do play a supporting role in hormonal health when deficiencies are present, no supplement replaces a proper medical evaluation. Marketing claims are not the same as clinical evidence, and self-managing symptoms with supplements while avoiding a real workup is a way of delaying answers rather than finding them.
Lifestyle as a Foundation, Not a Cure
Consistent, quality sleep is one of the most powerful levers most men have available for supporting hormonal health. Testosterone production is heavily concentrated during sleep, and chronic sleep restriction has a documented suppressive effect.
Resistance training - lifting weights, training for strength - supports testosterone and overall hormonal function in ways that cardiovascular exercise alone does not replicate.
Nutrition matters, particularly dietary fat, micronutrient adequacy, and managing excess body fat. Alcohol in significant quantities is a recognized suppressor of testosterone production and affects liver function, which circles back to SHBG. Chronic psychological stress keeps cortisol elevated, and elevated cortisol and healthy testosterone do not coexist easily.
None of this is presented as a simple fix. It is presented because these factors are real, they interact with each other, and they are within a man's control to influence - often before, during, or alongside any medical intervention.
What You Actually Need to Know Before Your Next Appointment
Total testosterone is a starting point. It is not a verdict. The amount of testosterone your body can actually use - free and bioavailable testosterone - is shaped by SHBG, albumin, your metabolic health, your age, your sleep, your stress levels, and other variables that a single standard lab value cannot capture.
Your symptoms are data. Your energy, your mood, your drive, your body composition, your sleep quality - these are not separate from your hormonal health. They are part of the evaluation.
A number without context is just a number. What matters is usable testosterone, how you feel, and the full clinical picture behind both. That is the standard of care that men actually deserve, and it is the approach that AlphaMD brings to every evaluation - looking at the complete hormonal picture, not just a single line on a lab report, with medically supervised care designed to give you real answers.
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
People are asking...
It makes no rational sense to me that total testosterone “far more important”…. even for starting dose. When subjects can have the same total testoste...
Maybe think of it a different way. Your FT level varies a lot based on your SHBG and your albumin levels. And since no one knows to what degree your body will respond to TRT, initial dosing, for the T... See Full Answer
I'm 37. I went to a clinic with my complaints and a hormonal test was done: Fsh 2.69mIU/mL Lh 7.28mIU/mL Prolactin 3.95ng/mL Testosterone 18.0nmol...
Your doctors didn’t lie in saying your labs don’t show anything abnormal. But they won’t always because what is “normal” is based on population averages, not what is normal for you. There is a new di... See Full Answer
I did a blood test in February and my doctor only had total testosterone tested. It came back as 339. I knew my doctor wouldn’t even consider prescrib...
So, providers on the AlphaMD platform utilize the updated age related treatment thresholds that were suggested in this study . If you are under age 45, a provider may determine that you qualify for t... See Full Answer
Get $30 off your first month’s order
Enter your email address now to receive $30 off your first month’s cost, other discounts, and additional information about TRT.
Legal Disclaimer
This website is a repository of publicly available information and is not intended to form a physician-patient relationship with any individual. The content of this website is for informational purposes only. The information presented on this website is not intended to take the place of your personal physician's advice and is not intended to diagnose, treat, cure, or prevent any disease. Discuss this information with your own physician or healthcare provider to determine what is right for you. All information is intended for your general knowledge only and is not a substitute for medical advice or treatment for specific medical conditions. The information contained herein is presented in summary form only and intended to provide broad consumer understanding and knowledge. The information should not be considered complete and should not be used in place of a visit, phone or telemedicine call, consultation or advice of your physician or other healthcare provider. Only a qualified physician in your state can determine if you qualify for and should undertake treatment.