Your Thyroid Is Sabotaging Your TRT (And Your Doctor Missed It)
Published on:
Updated on:
People are asking...
Age 62, athletic, nutrition freak (usa). Started TRT 15 months ago when testosterone at 298. Six months later it was 498 and I was doing great. Level ...
I'll share some conjecture here without knowing more. Taking everything at face value, I would say whatever medication you're taking might not be Testosterone Cypionate. When you take any Testosterone... See Full Answer
Been fighting with doctors and ins co for 30 years, chemo wiped out my ability to make test at the age of 18. I'm 52 now and I just take care of my me...
The fact that you have been fighting insurance tells me you are in the US. With that in mind, the main thing you need to be careful with self medicating is running afoul of the law. Going “legit” wou... See Full Answer
I've been on trt for about a year and it started right away, started at 160 a week and it was so bad I wouldn't be able to sleep for two days, but I'm...
RHR increase on TRT - while this is not a common complaint, it is known to occur. While the phenomenon has not been evaluated extensively, a common theory is that increased viscosity (thickness) of th... See Full Answer
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
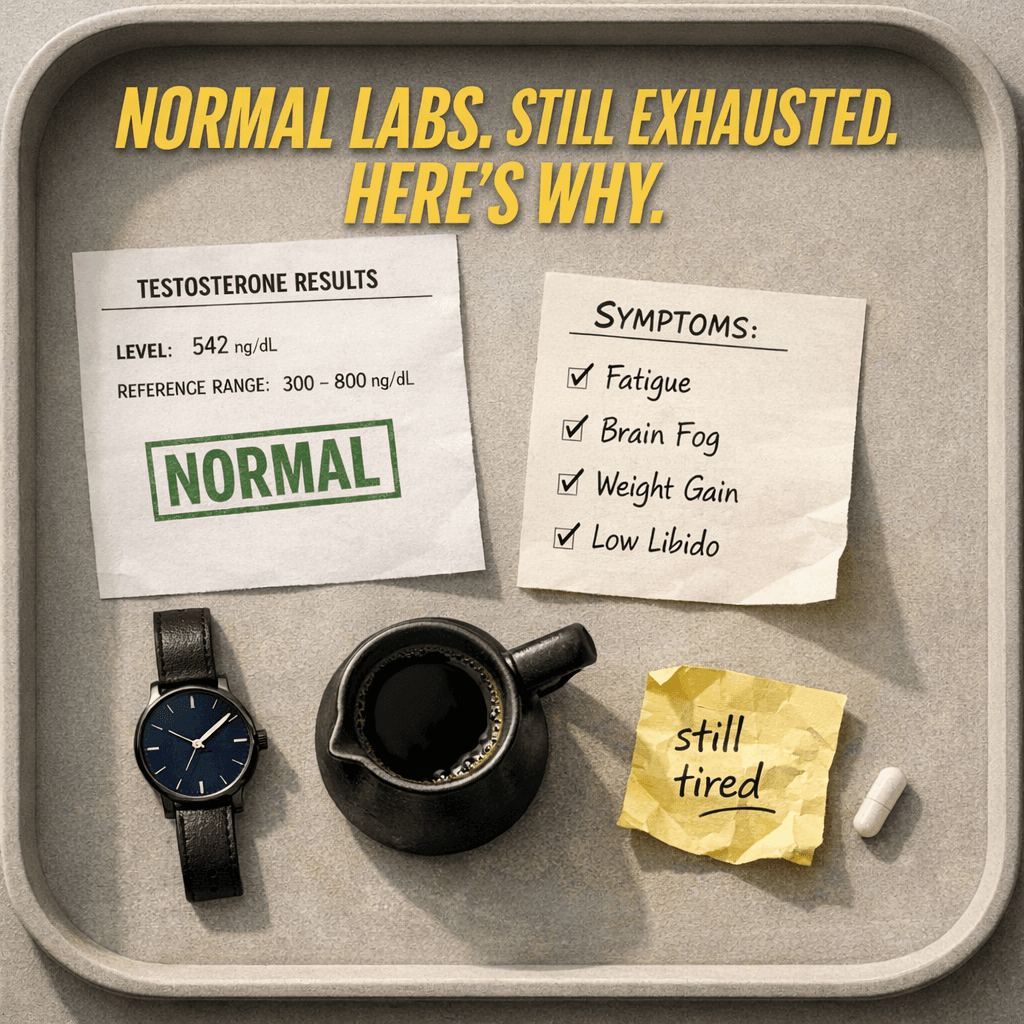
You've been on TRT for months, doing everything right, and you still feel like garbage. Your testosterone numbers look fine on paper, but the fatigue, the brain fog, the stubborn weight, the flat libido - none of it has budged the way you expected.
Before you assume your protocol needs tweaking, there's a possibility worth taking seriously: your thyroid may be quietly working against every benefit testosterone replacement is supposed to deliver.
The Hormone System Nobody Talks About in Men's Health Clinics
Testosterone gets most of the attention in men's hormone conversations, and for good reason. But testosterone doesn't operate in isolation. It exists inside a complex web of hormonal signals, and the thyroid sits at the center of that web in ways that most people, including some clinicians, underestimate.
The thyroid is a small, butterfly-shaped gland at the base of your throat, and it produces hormones that regulate how every cell in your body uses energy. When thyroid function is off, even slightly, the downstream effects can look almost identical to low testosterone. Fatigue, weight gain, low mood, poor libido, cold intolerance, sluggish recovery after exercise - the symptom lists overlap so significantly that one condition can mask the other for years.
For men already on TRT who aren't getting the results they expected, the thyroid is one of the first places a thorough clinician should look.
What TSH, Free T3, Free T4, and Reverse T3 Actually Mean
Thyroid testing is often reduced to a single number: TSH, or thyroid-stimulating hormone. TSH is produced by the pituitary gland and tells the thyroid to produce more hormone. When thyroid output is low, TSH rises. When it's high, TSH drops. It's a useful marker, but it's a signal from the pituitary, not a direct measurement of what your thyroid is actually delivering to your tissues.
Free T4 is the main hormone the thyroid secretes. It's largely inactive on its own and needs to be converted into free T3, the biologically active form that your cells actually use. That conversion happens primarily in the liver, kidneys, and gut, meaning your thyroid can be producing T4 just fine while poor conversion leaves your tissues relatively starved of active thyroid hormone.
Reverse T3, or rT3, is a mirror-image molecule of T3 that blocks T3 receptors without activating them. Under certain conditions - chronic stress, severe calorie restriction, illness, overtraining, inflammation - the body converts more T4 into reverse T3 instead of active T3. This is a protective mechanism, but in men pushing hard in the gym or under prolonged metabolic stress, it can create a functional thyroid deficiency even when TSH looks perfectly normal.
Thyroid antibodies are a separate but critical piece of the picture. Elevated TPO antibodies or anti-thyroglobulin antibodies signal autoimmune activity against the thyroid, a condition called Hashimoto's thyroiditis. It's not rare in men, though it's diagnosed far less often because it's rarely tested for unless symptoms are severe. Hashimoto's can cause thyroid function to fluctuate unpredictably, creating periods of hypothyroid symptoms that can be mistaken for hormonal imbalance or depression.
How a Struggling Thyroid Derails Testosterone - Even When Levels Are "Good"
Here's where the physiology gets genuinely interesting. Thyroid hormones directly influence several mechanisms that determine how well testosterone actually works in the body.
One of the most significant connections is through SHBG, or sex hormone-binding globulin. SHBG is a protein that binds to testosterone in the bloodstream, making it unavailable for use by tissues. Thyroid hormones influence SHBG production in the liver. Hypothyroidism tends to lower SHBG, which sounds beneficial at first, but the accompanying changes in how testosterone is metabolized often cancel out any advantage. Hyperthyroidism, on the other hand, can drive SHBG up significantly, leaving a man with total testosterone that looks fine while his free testosterone, the usable fraction, is genuinely low.
Thyroid dysfunction also affects aromatization, the process by which testosterone converts to estrogen. When thyroid function is impaired, this balance can shift, contributing to estrogen-related symptoms like water retention, mood instability, and reduced libido that men on TRT frequently misattribute to their protocol alone.
Beyond these hormonal mechanics, hypothyroidism impairs mitochondrial function, slows metabolic rate, disrupts sleep architecture, and blunts the anabolic signaling that makes muscle growth and fat loss possible. A man on TRT with subclinical hypothyroidism may find that he gains little muscle despite training consistently, holds onto body fat regardless of diet, and never quite feels the energy lift that testosterone replacement typically provides.
The Scenarios That Fall Through the Cracks
Consider a scenario that plays out more often than it should. A man in his forties starts TRT after labs confirm low testosterone. His numbers improve, he feels marginally better for a few weeks, and then the progress plateaus. His fatigue returns, his mood stays flat, and he gains weight around the midsection despite being careful with his diet. His clinician adjusts his testosterone dose, checks estrogen, considers adding other compounds. Nobody orders a full thyroid panel.
What eventually turns up: subclinical hypothyroidism and elevated TPO antibodies indicating early Hashimoto's. His TSH was technically within the standard reference range, so earlier basic screening had never flagged it. But in the context of his symptoms and his broader hormonal picture, his thyroid function was clearly not optimal for him.
This is one version of a very common story. Another involves men who overtrain or follow aggressive calorie deficits to improve body composition while on TRT. Severe restriction and high training loads suppress T3 through reverse T3 elevation. The result is a man doing everything he thinks he should be doing while his body is in a state of metabolic suppression that blunts every benefit TRT is supposed to provide.
Post-viral thyroid dysfunction is another scenario that has become more widely recognized in recent years. Viral illness can trigger transient or lasting thyroid inflammation, disrupting function in ways that take months to fully manifest. For men who started feeling worse after a significant illness, thyroid function is worth examining carefully.
"Normal" Labs and Why That Word Does a Lot of Heavy Lifting
The tension between what's statistically normal and what's optimal for an individual is real, and it matters for thyroid health just as much as it does for testosterone.
Lab reference ranges are calculated from population averages. A result that falls within the range means you're not dramatically outside what's typical for the general population. It doesn't mean your thyroid is functioning at the level your particular physiology needs to feel well and perform well. This is not a fringe position - it's a clinically relevant nuance that thoughtful endocrinologists and functional medicine practitioners navigate routinely.
This doesn't mean chasing numbers to extremes or assuming that any result in the lower part of a range warrants treatment. It does mean that for a man with persistent symptoms that align with thyroid dysfunction, a TSH in the normal range is not the end of the diagnostic conversation. Free T3, free T4, reverse T3, and antibody testing add meaningful context that TSH alone cannot provide.
The takeaway isn't that everyone's thyroid is broken or that every man on TRT needs thyroid medication. It's that symptom patterns matter, clinical context matters, and a single marker rarely tells the full story.
Nutrients, Medications, and Other Thyroid Disruptors Men Often Ignore
Several practical factors can interfere with thyroid function or lab accuracy in ways men on TRT may not connect to their symptoms.
Iodine is essential for thyroid hormone synthesis. Severe deficiency, uncommon in most developed countries but possible in men with very restricted diets, can impair production. Excessive supplemental iodine can paradoxically suppress thyroid function in susceptible individuals, which is why supplementing with high-dose iodine without medical guidance is not a straightforward solution. Selenium plays a supporting role in T4-to-T3 conversion and in protecting thyroid tissue from oxidative stress. Again, balance matters more than excess.
Certain medications and supplements can interfere with thyroid lab results or thyroid hormone absorption, including biotin supplements taken in high doses before blood draws, which can skew several lab values. Timing and consistency of blood draws matter as well. Testing thyroid markers under conditions of acute stress, illness, or immediately after an intense training cycle may not reflect your true baseline.
For men taking any medication regularly, a conversation with a clinician about potential thyroid interactions is a reasonable step, not an alarmist one.
When to Push for a Fuller Picture and When Endocrinology Belongs in the Conversation
If you're on TRT and not getting expected results, the right question to ask your clinician isn't just "should we adjust the dose?" It's worth discussing whether a comprehensive thyroid panel has been run, including free T3, free T4, reverse T3, and thyroid antibodies, not just TSH.
Symptom patterns that warrant this conversation include persistent fatigue that isn't improving with optimized testosterone, difficulty losing body fat despite reasonable effort, unexplained changes in cholesterol levels, cold sensitivity, hair thinning, mood or cognitive symptoms that don't fit the trajectory of TRT improvement, and libido or erectile issues that haven't responded to testosterone optimization.
For men whose thyroid abnormalities are complex, particularly those with confirmed autoimmune thyroiditis, significant antibody elevation, or symptoms that suggest fluctuating thyroid states, referral to an endocrinologist adds an important layer of expertise. There's no contradiction between working with a men's health clinic and involving a thyroid specialist when the clinical picture calls for it.
The misconception that thyroid conditions are primarily a concern for older women has real consequences for men. Thyroid dysfunction is underdiagnosed in men partly because it's under-suspected. Addressing it isn't a niche pursuit - it's basic endocrine due diligence.
The Full Picture Is the Only Picture That Works
TRT can be genuinely life-changing for the men who need it. But testosterone is not a stand-alone solution, and optimizing it in isolation while ignoring the broader hormonal environment is a bit like tuning an engine while leaving a clogged fuel line in place. The engine still won't run right.
Thyroid dysfunction, even when subtle, can undermine every goal that brings a man to TRT in the first place - energy, body composition, mood, sexual function, mental clarity, and training progress. The fact that it often hides behind "normal" lab values makes it easy to miss and easy to dismiss, which is exactly why it deserves more attention than it typically gets in men's health conversations.
With AlphaMD, the provider overseeing your care evaluates the full metabolic and endocrine picture, not just a single hormone in isolation. If you've been on TRT without getting the results you expected, the answer may not be a different dose. It may be a more complete conversation about everything that's happening in your body.
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
People are asking...
Age 62, athletic, nutrition freak (usa). Started TRT 15 months ago when testosterone at 298. Six months later it was 498 and I was doing great. Level ...
I'll share some conjecture here without knowing more. Taking everything at face value, I would say whatever medication you're taking might not be Testosterone Cypionate. When you take any Testosterone... See Full Answer
Been fighting with doctors and ins co for 30 years, chemo wiped out my ability to make test at the age of 18. I'm 52 now and I just take care of my me...
The fact that you have been fighting insurance tells me you are in the US. With that in mind, the main thing you need to be careful with self medicating is running afoul of the law. Going “legit” wou... See Full Answer
I've been on trt for about a year and it started right away, started at 160 a week and it was so bad I wouldn't be able to sleep for two days, but I'm...
RHR increase on TRT - while this is not a common complaint, it is known to occur. While the phenomenon has not been evaluated extensively, a common theory is that increased viscosity (thickness) of th... See Full Answer
Get $30 off your first month’s order
Enter your email address now to receive $30 off your first month’s cost, other discounts, and additional information about TRT.
Legal Disclaimer
This website is a repository of publicly available information and is not intended to form a physician-patient relationship with any individual. The content of this website is for informational purposes only. The information presented on this website is not intended to take the place of your personal physician's advice and is not intended to diagnose, treat, cure, or prevent any disease. Discuss this information with your own physician or healthcare provider to determine what is right for you. All information is intended for your general knowledge only and is not a substitute for medical advice or treatment for specific medical conditions. The information contained herein is presented in summary form only and intended to provide broad consumer understanding and knowledge. The information should not be considered complete and should not be used in place of a visit, phone or telemedicine call, consultation or advice of your physician or other healthcare provider. Only a qualified physician in your state can determine if you qualify for and should undertake treatment.