Can I Start TRT at 450? Understanding Testosterone Therapy in the "Normal" Range
Published on:
Updated on:
People are asking...
180 being a bit high for a start would you recommend lower dosing? Without looking at my labs, are you saying it’s more common to start off around 150...
Without getting too specific, or try to guide your treatment, I will just say that the majority of men on TRT in the US average between 100-140mg/wk. The medical textbook standard is currently to star... See Full Answer
What is the normal level of testosterone for healthy males? My doctor says it is 300....
The idea of normal ranges is not a good one. It is a very subjective level for each man. That said, 300 is the lower end of the insurance based "normal ranges" and really just refers to where insuranc... See Full Answer
What levels do you consider low enough that the person will see a benefit from TRT?...
In general, it's a lot more about how someone feels than about the numbers themselves. The range for "acceptable" Testosterone in men can go from 250-1000. That's honestly crazy for any other hormone ... See Full Answer
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
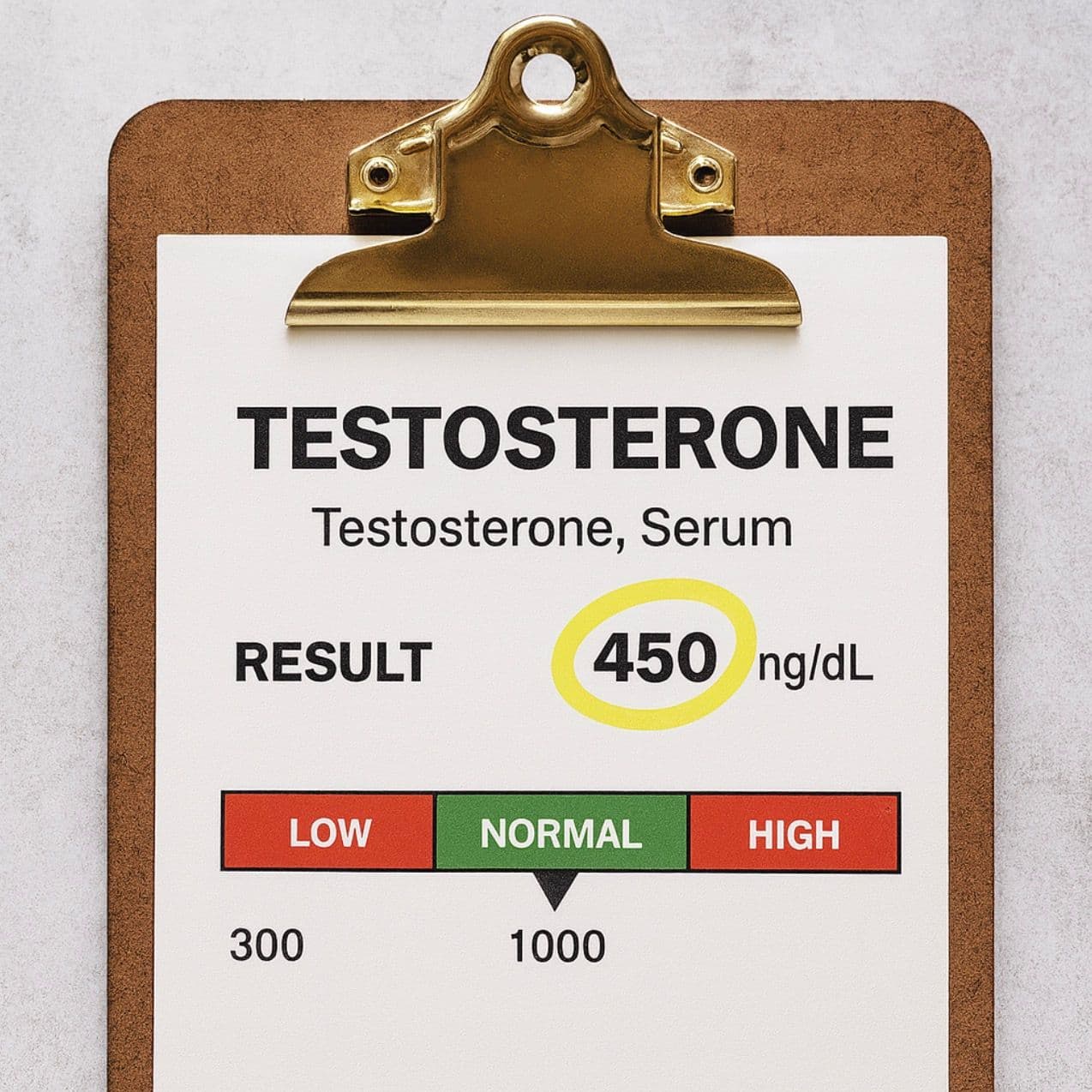
If you've landed on this article, there's a good chance you're frustrated. Your testosterone came back at 450 ng/dL—solidly in the "normal" range according to the lab report—but you feel anything but normal. Maybe you're dragging through the afternoon, your libido has disappeared, or brain fog has become your constant companion. You bring this up to your doctor, and they tell you everything looks fine. "Your levels are normal," they say, offering to prescribe antidepressants instead. So you start researching Testosterone Replacement Therapy (TRT) online, wondering if this could be the answer.
Sound familiar?
The question "Can I start TRT at 450?" isn't just about a number on a lab report. It's about whether you should accept feeling mediocre when you could potentially feel great. Let's explore this controversial topic with the nuance it deserves.
The Problem with "Normal"
Here's something most doctors won't tell you: the testosterone reference range of 250-900 ng/dL (or sometimes 264-916 ng/dL, depending on the lab) is based on a statistical average of the male population. That population includes 80-year-old men, men with chronic illnesses, men who are obese, and yes, healthy young men too.
Think about that for a second. If you're 35 years old and your testosterone is 450 ng/dL, you might be "normal" compared to a 70-year-old man. But is that really where you want to be?
The reference range tells you what's statistically average, not what's optimal for you. There's a massive difference between these two concepts, and this distinction is at the heart of the controversy around starting TRT in the "normal" range.
Why Doctors Often Say No
Before we go further, it's worth understanding why many physicians are hesitant to prescribe TRT when your levels are above 300-350 ng/dL. It's not always because they don't care—there are legitimate reasons for their caution:
1. Insurance and Liability Concerns
Most insurance companies have strict cutoffs, often requiring testosterone levels below 300 ng/dL for coverage. If your doctor prescribes TRT at 450 ng/dL, you're paying out of pocket, and they're potentially opening themselves up to scrutiny about prescribing outside standard guidelines.
2. Outdated Guidelines
Many physicians follow clinical practice guidelines that were established years ago when the understanding of testosterone's role was less sophisticated. These guidelines often use hard cutoffs rather than symptom-based approaches.
3. Lack of Specialization
Your primary care doctor sees patients with diabetes, heart disease, respiratory issues, and hundreds of other conditions. Hormone optimization isn't their specialty, and they may not be comfortable managing the nuances of TRT.
4. Genuine Concern About Long-Term Commitment
TRT is typically a lifelong commitment. Once you start, your body's natural production shuts down. Some doctors genuinely worry about starting young, otherwise healthy men on a medication they'll need to take forever.
These aren't bad reasons. They're just not the whole picture.
The Case for Starting TRT at 450
Now let's look at the other side—because there's a growing body of evidence and clinical experience suggesting that for many men, 450 ng/dL isn't sufficient.
Symptoms Matter More Than Numbers
Here's a revolutionary concept: medicine should treat the patient, not the lab value.
If you have a testosterone level of 450 ng/dL but you're experiencing:
- Persistent fatigue that sleep doesn't fix
- Significant reduction in libido
- Erectile dysfunction or diminished sexual performance
- Brain fog and concentration problems
- Loss of muscle mass despite training
- Increased body fat, particularly around the midsection
- Depression or lack of motivation
- Loss of morning erections
Then your testosterone level is too low for you, regardless of what the reference range says.
Providers have worked with 30-year-old men who started TRT with testosterone in the 400-500 range and experienced dramatic improvements within weeks. Morning erections returned. Brain fog lifted. The gym sessions that felt like pushing through concrete suddenly felt effortless again. These weren't placebo effects—these were men getting their vitality back.
The Age Factor
Context matters enormously. A 450 ng/dL testosterone level means very different things for different men:
- For a 70-year-old man: This is actually quite good
- For a 25-year-old man: This is concerning and worth investigating
- For a 35-year-old man: This is borderline and warrants a symptom-based evaluation
- For a 50-year-old man: This might be acceptable if he feels good, or problematic if he doesn't
A healthy man in his 20s and 30s should typically have testosterone levels well above 500 ng/dL, often in the 600-900 range. If you're 32 years old with a testosterone level of 450, you're already operating below what would be expected for your age.
The Free Testosterone Piece of the Puzzle
Here's something critical that many doctors miss: Total testosterone isn't the whole story. What really matters is your free (bioavailable) testosterone—the testosterone your body can actually use.
You could have a total testosterone of 600 ng/dL and still have symptoms if your sex hormone binding globulin (SHBG) is elevated. SHBG binds to testosterone and makes it unavailable for your tissues to use. Some men have naturally high SHBG, which means even with "normal" total testosterone, their free testosterone is in the gutter.
Some patients have total testosterone in the 500s but free testosterone below the reference range because their SHBG is sky-high. When their provider started them on TRT and brought their total testosterone to 900-1000 ng/dL, their free testosterone finally reached optimal levels, and they felt dramatically better.
Bottom line: If your doctor only checked total testosterone and is making decisions based solely on that number, you're not getting the full picture. Free testosterone and SHBG should always be part of the evaluation.
Real Patient Experiences
Here are some anonymized patient experiences that illustrate how this can play out:
Case 1: Jake, Age 30
- Initial total testosterone: 470 ng/dL
- Symptoms: No libido, erectile dysfunction, severe brain fog, sleeping 10 hours and still exhausted
- Doctor's response: "You're in the normal range. Maybe try therapy for the stress."
- Started TRT at 140mg/week after seeking a second opinion
- Result: Within 2 weeks, morning erections returned. Within 6 weeks, brain fog completely cleared, energy normalized, and libido came back strong.
- His reflection: "I didn't realize how bad I felt until I felt good again."
Case 2: Marcus, Age 42
- Initial total testosterone: 445 ng/dL, free testosterone at the very bottom of the range
- Symptoms: Moderate fatigue, difficulty building muscle, declining motivation
- Tried lifestyle changes first: improved sleep, added strength training, optimized diet
- Retested after 3 months: total testosterone improved to 510 ng/dL
- Decision: Continued without TRT, symptoms improved enough that he felt it wasn't necessary
- His reflection: "I'm glad I tried the natural route first. It wasn't a miracle cure, but I feel better enough that I want to see how far lifestyle can take me."
Case 3: David, Age 38
- Initial total testosterone: 425 ng/dL
- Started TRT through an online clinic at 200mg/week
- Initial result: Felt amazing for about 6-8 weeks
- Long-term result: Developed significant water retention, elevated estrogen, required AI, hematocrit went to 52%
- Adjusted down to 120mg/week with better injection frequency
- Current status: Feels great without the side effects, wishes he'd started at a lower dose
These stories illustrate something important: starting TRT at 450 ng/dL can be life-changing for some men, but it's not automatic, and the approach matters enormously.
When You Should Try Lifestyle Optimization First
Before committing to lifelong TRT, there are situations where it makes sense to try optimizing your natural production first:
You should consider lifestyle changes first if:
- You're overweight or obese. Fat tissue contains aromatase enzyme, which converts testosterone to estrogen. Losing 30-50 pounds can significantly increase testosterone levels.
- Your sleep is poor. Testosterone is primarily produced during deep sleep. If you're sleeping 5-6 hours a night or have untreated sleep apnea, fixing this can dramatically improve testosterone.
- You're chronically stressed with high cortisol. Chronic stress directly suppresses testosterone production. Sometimes the answer isn't TRT—it's changing your stressful job or addressing anxiety.
- Your diet is terrible. Severe caloric restriction, very low-fat diets, and nutrient deficiencies can tank testosterone. Sometimes eating more and better is the answer.
- You're not exercising at all. Resistance training and high-intensity exercise can naturally boost testosterone production.
- You're taking medications known to lower testosterone. Opioids, certain antidepressants, and other medications can suppress testosterone. Sometimes switching medications solves the problem.
The reasonable approach: give lifestyle optimization 3-4 months with dedicated effort. Retest your testosterone. If you've made substantial improvements but still feel symptomatic, or if you made all the changes and your testosterone barely budged, then TRT makes more sense.
When TRT at 450 Makes Sense
On the flip side, there are situations where starting TRT at 450 ng/dL is entirely reasonable:
Consider starting TRT at 450 if:
- You're young (under 40) and symptomatic. A 28-year-old shouldn't feel like a 58-year-old. If you've ruled out other causes and you're significantly symptomatic, age matters.
- Your free testosterone is low despite normal total testosterone. This is the SHBG issue we discussed earlier. If your bioavailable testosterone is insufficient, the total number doesn't tell the full story.
- You've tried legitimate lifestyle interventions for 3-6 months without improvement. If you've cleaned up your diet, you're sleeping well, you've lost weight, you're training hard, and you still feel terrible with a testosterone of 450, continuing to suffer doesn't make you noble—it just makes you miserable.
- You have clear symptoms significantly impacting quality of life. If you can't perform sexually, you're profoundly fatigued, and it's affecting your relationships and career, quality of life matters.
- You've had your testosterone checked multiple times over months and it's consistently in the 400-500 range. One low reading could be a fluke (illness, poor sleep the night before, time of day). Consistently low readings are more meaningful.
- Other causes of your symptoms have been ruled out. Make sure you're not actually dealing with thyroid disease, vitamin D deficiency, anemia, depression from other causes, or other medical conditions that can mimic low testosterone.
The "Optimization vs. Replacement" Ethical Question
Here's where things get philosophically interesting: Is starting TRT at 450 ng/dL true hormone replacement therapy, or is it actually hormone optimization therapy?
True replacement therapy means you're replacing something that's deficient. If your testosterone is 150 ng/dL, you clearly have hypogonadism. No one debates that.
But at 450 ng/dL, you're technically not deficient by standard medical definitions. You're choosing to optimize your levels beyond what your body is currently producing to achieve better functioning.
Is this wrong? I don't think it's a simple yes or no.
Consider this: Doctors don't hesitate to give thyroid medication to people with subclinical hypothyroidism if they're symptomatic. They treat vitamin D levels of 30 ng/mL even though that's technically "sufficient" because optimal levels are known to be higher. They prescribe ADHD medications to adults who functioned fine but functioned better with treatment.
Medicine is increasingly moving toward optimization, not just treating overt disease. The question isn't whether optimization is ethical—it's whether the benefits outweigh the risks and whether the patient is making an informed decision.
That said, you need to go into this with eyes wide open:
- You're committing to lifelong treatment. Your natural production will shut down. If you stop TRT later, you may not return to your starting point—you might end up lower.
- You're accepting some health monitoring requirements. You'll need regular bloodwork to monitor hematocrit, lipids, liver function, and other markers.
- There are risks. Cardiovascular effects, fertility concerns, potential for dependency, and other factors need to be part of your decision.
- You might not feel as dramatically better as you hope. If your symptoms aren't primarily testosterone-related, TRT won't be a magic cure.
How Providers at AlphaMD Approach This Question
The licensed providers you'll meet through AlphaMD don't use arbitrary cutoffs. They don't say "No TRT unless you're below 300" or "Everyone with symptoms gets TRT regardless of levels."
Here's how a provider approaches it when someone comes to AlphaMD with testosterone in the 450 range:
1. Comprehensive Testing
Your provider checks total testosterone, free testosterone, SHBG, estradiol, LH, FSH, thyroid panel, vitamin D, and other relevant markers. The goal is the full picture, not just one number.
2. Symptom Assessment
Licensed providers use validated questionnaires and detailed discussions to understand how you're actually feeling and functioning, not just what your labs say.
3. Rule Out Other Causes
Before attributing everything to testosterone, the provider makes sure thyroid issues, sleep disorders, nutrient deficiencies, and other treatable conditions aren't being missed.
4. Individualized Decision-Making
A 25-year-old with testosterone of 450 gets a different conversation than a 55-year-old with the same number. Your age, goals, symptom severity, and overall health all factor into the recommendation.
5. Trial Period if Appropriate
Sometimes the provider recommends lifestyle interventions first with a recheck in 3 months. Sometimes the symptom severity warrants starting treatment. You make this decision together with your provider.
6. If Your Provider Starts TRT, It's Done Right
Unlike cookie-cutter clinics that start everyone at 200mg/week, providers typically start at lower doses (100-140mg/week for most men) and adjust based on your response. They don't automatically prescribe AI (aromatase inhibitors) unless bloodwork and symptoms indicate it's needed. They monitor carefully and adjust as needed.
Questions to Ask Yourself
Before making your decision, work through these questions honestly:
- Have I truly optimized my lifestyle? (Sleep, nutrition, exercise, stress management, body composition)
- Have I ruled out other medical causes of my symptoms? (Thyroid, vitamin deficiencies, sleep apnea, depression from other causes)
- Are my symptoms severe enough to justify lifelong treatment? (Minor complaints vs. significant quality of life impact)
- Do I understand this is likely a permanent decision? (Natural production may not fully recover if I stop)
- Am I prepared for the monitoring and adjustment process? (Regular bloodwork, possible side effect management, finding optimal dosing)
- Am I doing this for the right reasons? (Legitimate symptom relief vs. hoping for performance enhancement when I'm actually fine)
- Have I checked free testosterone, not just total? (Understanding if my testosterone is actually bioavailable)
- Is my decision being influenced by TRT marketing? (Genuine need vs. social media/clinic advertising making me think I need it)
The Bottom Line
So, can you start TRT at 450?
The honest answer: It depends.
If you're a 28-year-old man with severe symptoms, free testosterone in the tank, and you've tried lifestyle interventions without success—then yes, TRT can be entirely appropriate and potentially life-changing.
If you're a 55-year-old man with mild symptoms who hasn't tried improving sleep, losing weight, or addressing stress—then maybe hold off and try those interventions first.
The number 450 doesn't exist in a vacuum. It exists in the context of:
- Your age
- Your symptoms and their severity
- Your free testosterone and SHBG
- Whether other treatments might help
- Your personal values about optimization vs. accepting natural aging
- Your understanding of the commitment involved
One thing is definite: you're not crazy for feeling terrible at 450 ng/dL. The "normal range" doesn't mean you should accept feeling mediocre. At the same time, TRT isn't a decision to make lightly or rush into without trying other options first.
Moving Forward
If you're considering TRT with testosterone around 450:
- Get comprehensive testing. Don't make decisions based on total testosterone alone.
- Find a knowledgeable provider. Work with someone who understands hormone optimization, not just cookie-cutter protocols.
- Try legitimate lifestyle interventions if you haven't already, and give them a fair shot (3-4 months minimum).
- Don't let anyone dismiss your symptoms just because you're "in range."
- Don't let anyone pressure you into treatment if you're not sure it's right for you.
- Educate yourself on what to expect, both the benefits and the potential downsides.
- If you start TRT, do it right: appropriate dosing, proper monitoring, and willingness to adjust based on how you respond.
The goal isn't just to get your testosterone number higher—it's to help you feel better, function optimally, and live a fuller life. For some men at 450 ng/dL, TRT is the path to that goal. For others, different interventions make more sense. The key is making an informed decision based on your individual situation, not arbitrary numbers or one-size-fits-all rules.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Testosterone therapy should only be started under the supervision of a qualified healthcare provider. Individual results and experiences with TRT vary significantly. What works for one person may not work for another, and all medical decisions should be made in consultation with your healthcare provider based on your specific situation, comprehensive testing, and thorough evaluation.
If you're experiencing symptoms of low testosterone and want to work with a provider who takes an individualized, symptom-based approach rather than relying on arbitrary cutoffs, AlphaMD is here to help. We believe in comprehensive testing, care that treats the patient (not just the number), and providers who find your optimal protocol—not cookie-cutter solutions.
Have a question? Ask us.
At AlphaMD, we're here to help. Feel free to ask us any question you would like about TRT, medical weightloss, ED, or other topics related to men's health. Or take a moment to browse through our past questions.
People are asking...
180 being a bit high for a start would you recommend lower dosing? Without looking at my labs, are you saying it’s more common to start off around 150...
Without getting too specific, or try to guide your treatment, I will just say that the majority of men on TRT in the US average between 100-140mg/wk. The medical textbook standard is currently to star... See Full Answer
What is the normal level of testosterone for healthy males? My doctor says it is 300....
The idea of normal ranges is not a good one. It is a very subjective level for each man. That said, 300 is the lower end of the insurance based "normal ranges" and really just refers to where insuranc... See Full Answer
What levels do you consider low enough that the person will see a benefit from TRT?...
In general, it's a lot more about how someone feels than about the numbers themselves. The range for "acceptable" Testosterone in men can go from 250-1000. That's honestly crazy for any other hormone ... See Full Answer
Get $30 off your first month’s order
Enter your email address now to receive $30 off your first month’s cost, other discounts, and additional information about TRT.
Legal Disclaimer
This website is a repository of publicly available information and is not intended to form a physician-patient relationship with any individual. The content of this website is for informational purposes only. The information presented on this website is not intended to take the place of your personal physician's advice and is not intended to diagnose, treat, cure, or prevent any disease. Discuss this information with your own physician or healthcare provider to determine what is right for you. All information is intended for your general knowledge only and is not a substitute for medical advice or treatment for specific medical conditions. The information contained herein is presented in summary form only and intended to provide broad consumer understanding and knowledge. The information should not be considered complete and should not be used in place of a visit, phone or telemedicine call, consultation or advice of your physician or other healthcare provider. Only a qualified physician in your state can determine if you qualify for and should undertake treatment.